An introduction to EBM (session 1)
Session outline
This session aims to introduce the theory and practice of evidence-based health and care practice.
- we’ll begin with a simple introduction to evidence-based medicine (EBM)
- we’ll then work through a series of exercises
- to show both the problems that EBM solves, and the methods it uses to solve them
- we’ll introduce a mini-guide to finding, appraising, and reading a paper
- then taking what you’ve learned, and making a decision
- then we’ll set up a core EBM topic: the ranking of evidence
- and we’ll finish by looking at the wider EB* family, of which EBM is just one member
Exercises
- E1: find a paper
- E2: the EBM way
- E3: bias, confounding, and effect sizes
- E4: a mini-appraisal
- E5: your EB*
Introduction
The sentence
Evidence-based medicine (EBM) is the:
“conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients” (Sackett et al. 1996)
Meaning?
EBM as a set of standards for making decisions in medicine:
- conscientious: using evidence wherever possible
- explicit: naming the evidence that you’ve relied on to make a decision
- judicious: applying standards to judge that evidence
So what?
“arguably the most important movement in medicine in the past 25 years” (Smith 2015)
EBM’s domain
- clinical
- individual care
- “current best”
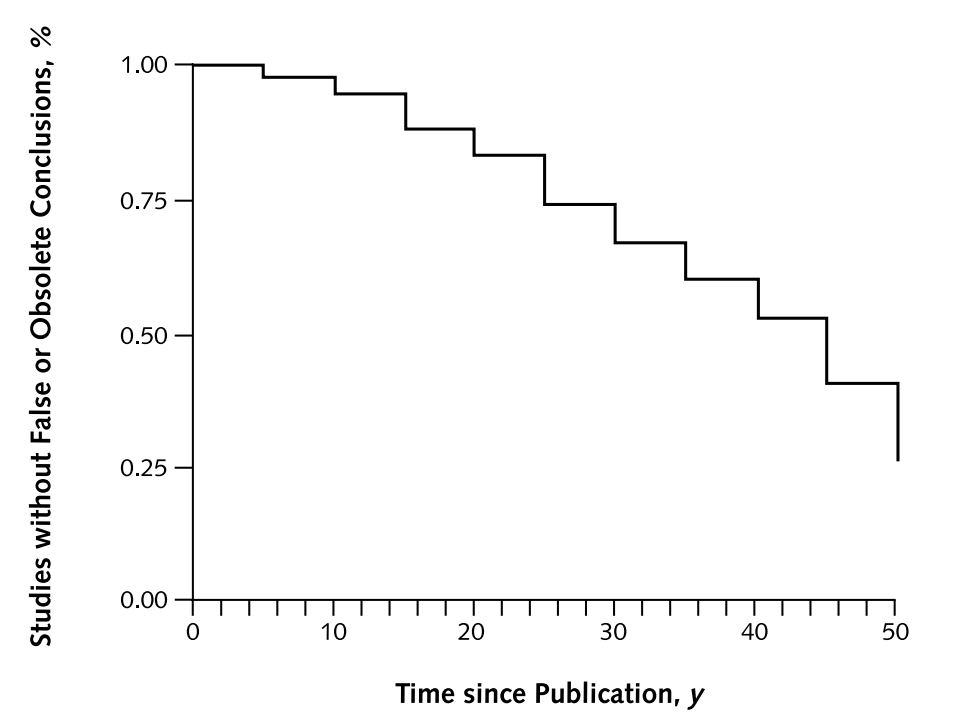
The half-life of facts
Finding papers
E1: find a paper
- go to the Knowledge Network home page
- find a paper about your area of work
- spend three minutes having a look at the paper
- please share one conclusion / takeaway from it in the chat
The takeaway from E1: papers are hard!
It’s often not very obvious how a paper should change our practice. Papers are often:
- complicated, poorly written, annoying…
- fallible
- excessively abstract
- deal with unfamiliar problems
- make many suggestions
EBM gives us rules for reading papers, and acting on what they say.
Appraising papers
The sentence
Evidence-based medicine (EBM) is the:
“conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients” (Sackett et al. 1996)
Reacting against non-systematic approaches to using evidence to make decisions.
What happened before EBM?
This is now really one for the historians of medicine, because we’re talking about c.1995 or before. But many of the early EBM proponents have written about what they felt was wrong with what came before. For example, this video by Guyatt sets it out especially clearly as a combination of physiologic rationale, practical experience, listening to authorities, rather than anything based on the relevant research.
Physiologic rationale
When clinicians had a patient with a problem and they weren’t sure of what to do, they would rely on 3 things. Number one, they would rely on physiologic rationale. They would think about the physiologic situation and they would make deductions on the basis of their understanding of the physiology. (All about EBM)
Practical experience
Then they would think of practical experience. They would think of their own practical experience, what happened when they saw patients like this before and when they tried this and that and see what happens. And they would think about that. (All about EBM)
Not the research!
It would never occur to anybody to go to the original literature. And if they did go to the original literature, they would have no idea how to distinguish what was trustworthy from what was untrustworthy. And that was the way the world was. (All about EBM)
EBM methods give us a system for using evidence to make decisions
- having a system simplifies that journey from evidence to decision
- picking out which research we can trust
- showing us which conclusions we should incorporate into our practice
- subtly, suggesting that we go from decision to evidence, rather than absorbing all the evidence then making decisions
E2: the EBM way
- please reflect on the reasons that you might trust or distrust the paper that you found in E1
- please put a reason to trust the paper, and a reason to distrust it, into the chat
Narrowing the scope of inquiry
EBM helps narrow the pool of things that we need to engage with/worry about. For example, when we come to talk about Greenhalgh’s approach to reading papers (Greenhalgh 2019), we’ll see attention paid to the following especially-salient issues:
- methods
- was the trial randomised?
- were the pre-trial groups similar?
- apart from treatment, were the groups treated similarly?
- was anyone lost to follow-up?
- was there appropriate masking?
- effects
- how large was the effect?
- how precisely was the effect measured?
- relevance
- are the results relevant to my practice?
That’s not the only way of understanding what we should pay attention to. In fact, one of the challenges in EBM is that different authors have different ideas about what exactly we should worry about. But in very general terms, we can usually identify three central concerns that crop up across EBM as a whole.
Three central concerns in EBM
- bias
- confounding
- effect sizes
Bias in general is boring
- AKA “systematic error”
“We define bias as…deviation from the truth” (Boutron et al. 2023)
Specific biases are fascinating
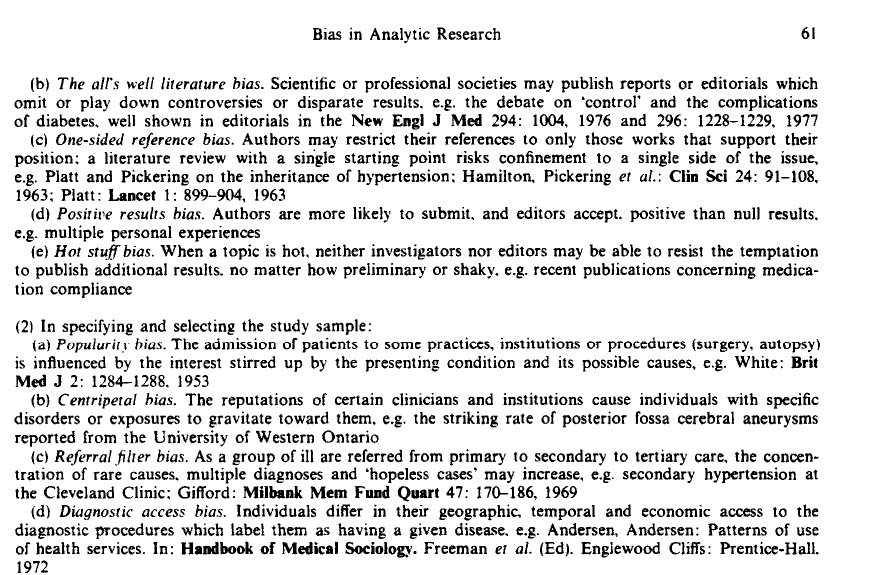
Specific biases are fascinating
- CEBM’s catalogue of biases
- EBM in very broad terms tries to minimise important biases
Confounding is probably the most important bias
What we think is happening
What’s actually happening 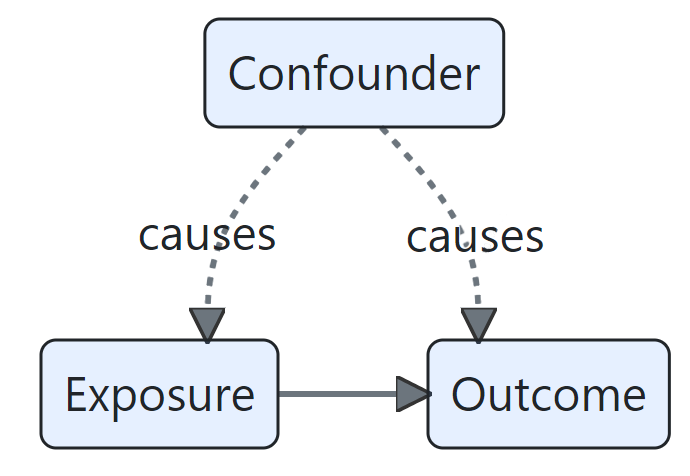
E3: bias, confounding, and effect sizes
- take a look at this plot of coronary artery disease rates:
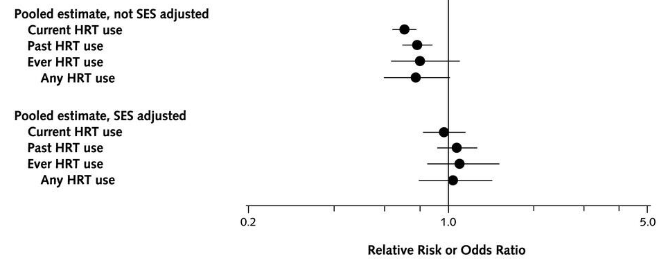
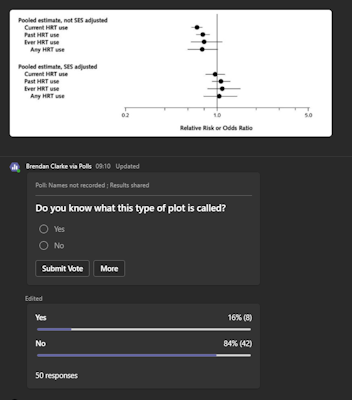
- what type of plot is this?
- how would you explain the main finding here in simple terms?
- what might explain the difference between the two groups?
Confounding and coffee
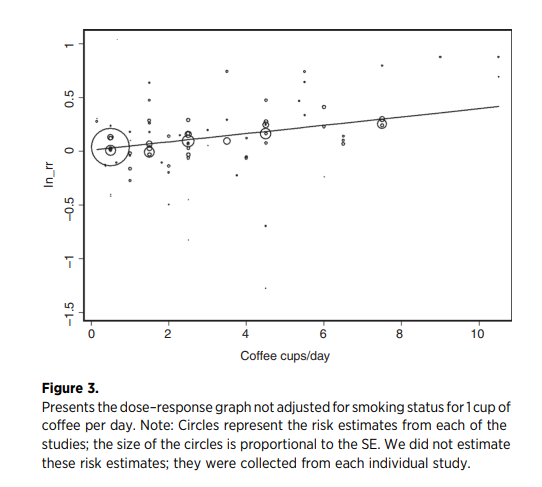
when the potential confounding effect from smoking is controlled for, coffee drinking does not appear to be a lung cancer risk factor (Galarraga and Boffetta 2016)
Thanks to Noora Salem (NHS GGC) for this example
Blobbograms (or forest plot)
Guarding against bias through judgement
- the core EBM methods are specifically designed to guard against bias and confounding
- randomisation ensures that different groups are comparable
- masking ensures fair measurement of effects
- reporting how individuals were followed-up prevents distorting results
- also provide a standard set of tools for expressing effect sizes
- for instance, the use of confidence intervals
- we’ll do this conscientiously by appraising each piece of evidence in the same way
The appraisal
E4: a mini-appraisal
- open the Oxford Centre for Evidence-Based Medicine RCT Critical Appraisal Sheet
- spend three minutes reading through
- please re-report a finding from the paper from E1 using the critical appraisal sheet - put your finding in the chat
From appraisal to ranking
- because EBM introduced methods for appraising evidence, this gave rise to a ranking of kinds of evidence
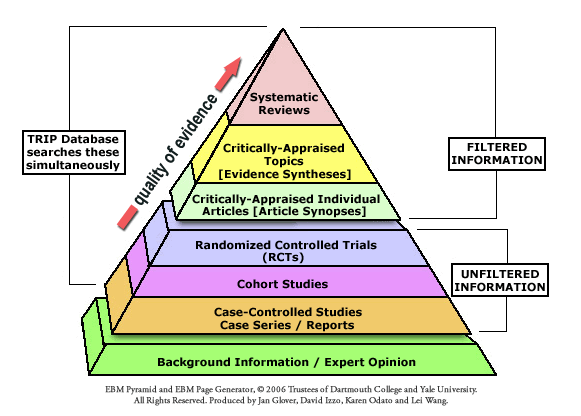
- that ranking of evidence will be a core topic for us in session 3
Beyond the care of the individual patient
- EBM originally was about making individual clinical decisions about treatment from published research evidence
- that scope has widened enormously over the past 30 years:
- to non-clinical domains of practice
- to guide the management of groups rather than individuals
- to support decisions about non-treatment questions
- to encompass other types of evidence
E5: your EB*
- in the chat, please give us a few words on these two questions:
- where can you see the conscientious, judicious, and explicit use of current best evidence in your practice?
- are there any areas of your practice that are not evidence-based in this way?
Beyond the individual paper
- just as the scope of EBM has changed over time, we’ll also see how the methods of EBM have changed too
- part of that reflects the widening of scope
- part of that is down to changes in publication practices
- part of that is down to changes in methodological emphasis
This means that very different practices have flown under the EBM banner at different times and in different places. To avoid contradictions, we’ll endorse a single coherent set of recommendations in this course, drawn from Greenhalgh (2019).
…and beyond the sentence
Evidence-Based Medicine is the integration of best research evidence with clinical expertise and patient values. (Sackett et al. 2000)
Next time!
- in the next session, we’ll look specifically at the most important trial methodology: the randomised control trial
- that will set us up to think more carefully about bias and confounding, particularly as they relate to published evidence
- that will set us up nicely for the next-next session, where we’ll put that core EBM approach to work, and appraise a paper of our own